| Specimen | Name | Result | Units | Range | ||||||||||||
| Plasma | Sodium | 144 | mmol/L | (135-145) | ||||||||||||
| Potassium | 1.7 | mmol/L | (3.5-5.5) | |||||||||||||
| Chloride | 85 | mmol/L | (100-109) | |||||||||||||
| Bicarbonate | 40 | mmol/L | (22-32) | |||||||||||||
| Urea | 3.4 | mmol/L | (2.7-7.2) | |||||||||||||
| Creatinine | 80 | μmol/L | (60-110) | |||||||||||||
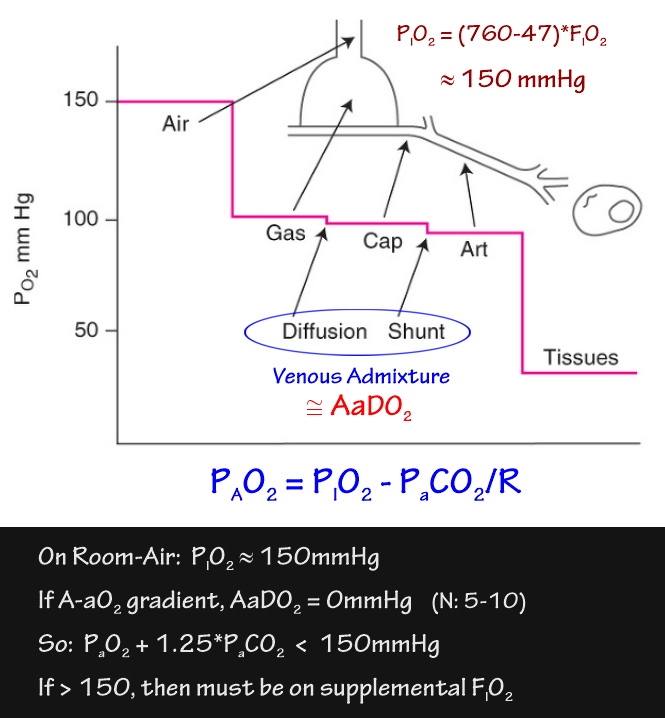
| ABG | pH | 7.56 | (7.36-7.44) | |||||||||||||
| PaO2 | 68 | mmHg | (70-100) | |||||||||||||
| PaCO2 | 44 | mmHg | (35-45) | |||||||||||||
| HCO3- | 38 | mmol/L | (21-26) | |||||||||||||
| Urine | Sodium | 22 | mmol/L | (> 20) | ||||||||||||
| Chloride | 84 | mmol/L | ||||||||||||||
| Creatinine | 71 | μmol/L | ||||||||||||||
|
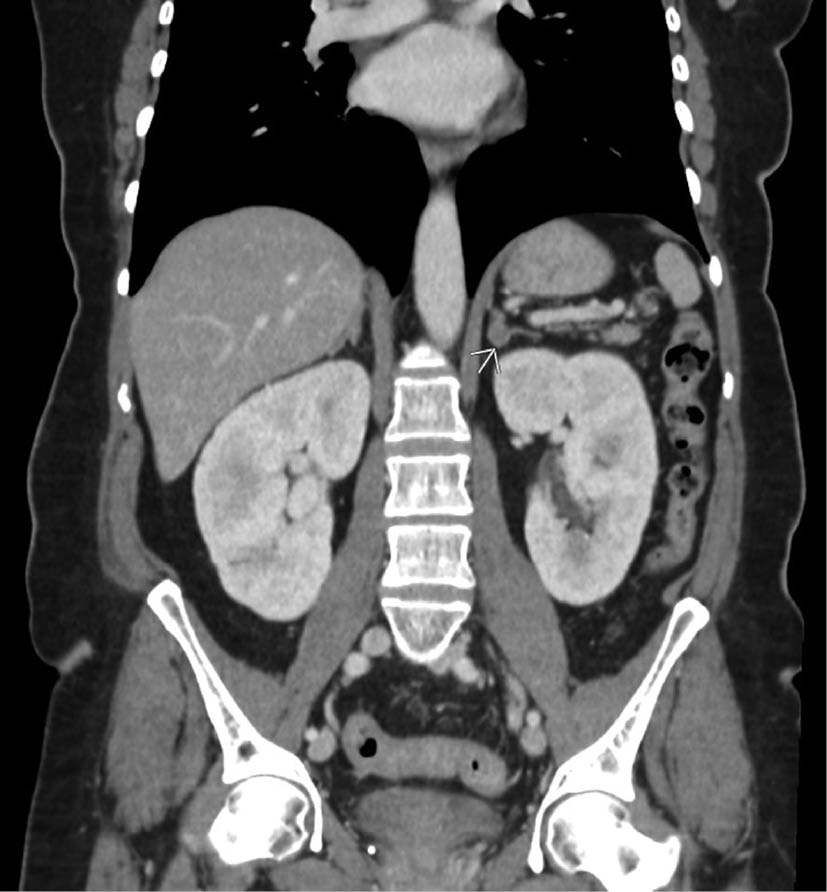
Adult patient with persistent hypertension. |
||||||||||||||||
Primary Hyperaldosteronism
Conn's Syndrome - benign adenoma of the zona glomerulosa of the adrenal cortex
|
||||||||||||||||
{kind=link}
{kind=link}