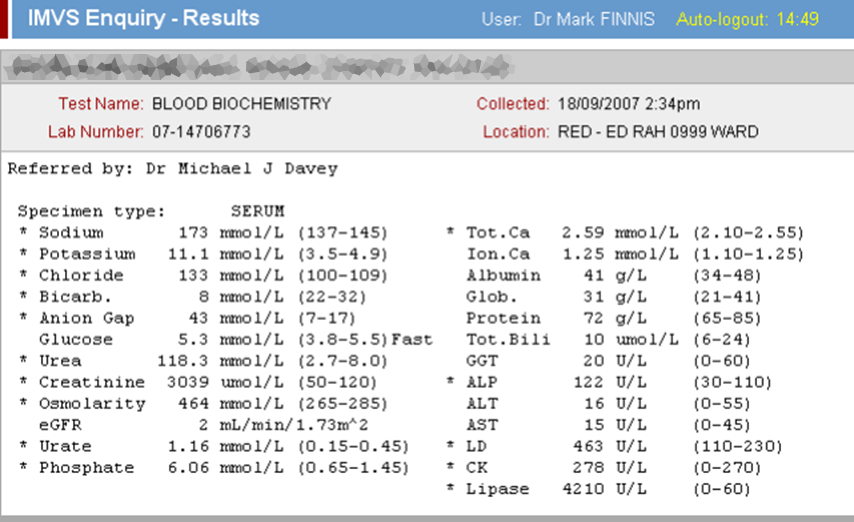
| Specimen | Name | Result | Units | Range |
| Plasma | Sodium | 173 | mmol/L | (135-145) |
| Potassium | 11.1 | mmol/L | (3.5-5.5) | |
| Chloride | 133 | mmol/L | (100-109) | |
| Bicarbonate | 8 | mmol/L | (22-32) | |
| Anion Gap | 43 | mmol/L | (7-17) | |
| Glucose | 5.3 | mmol/L | (3.8-5.5) | |
| Urea | 118 | mmol/L | (2.7-7.2) | |
| Creatinine | 3,039 | μmol/L | (60-110) | |
| Osmolality | 464 | mmol/kg | (275-295) | |
| Urate | 1.16 | mmol/L | (0.20-0.40) | |
| Phosphate | 6.06 | mmol/L | (0.80-1.45) | |
| Total Calcium | 2.59 | mmol/L | (2.10-2.55) | |
| Ionized Calcium | 1.25 | mmol/L | (1.07-1.27) | |
| Albumin | 41 | g/L | (34-48) | |
| Globulins | 31 | g/L | (22-35) | |
| Total Protein | 72 | g/L | (60-80) | |
| Total Bilirubin | 10 | μmol/L | (6-24) | |
| GGT | 20 | U/L | (< 60) | |
| ALP | 122 | U/L | (30-110) | |
| ALT | 16 | U/L | (< 55) | |
| AST | 15 | U/L | (< 45) | |
| LDH | 463 | U/L | (110-230) | |
| Lipase | 4,210 | U/L | (< 60) | |
| CK | 278 | U/L | (< 200) | |
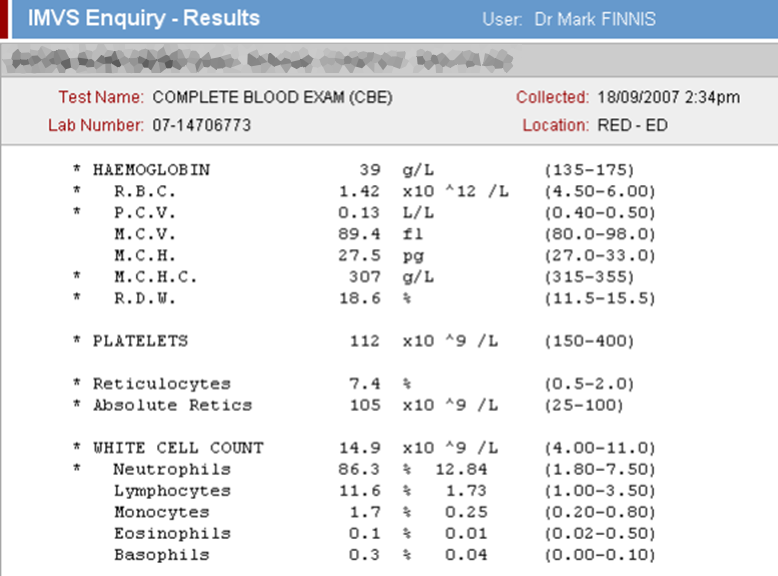
| Blood | Hb | 39 | g/L | (130-180) |
| Platelets | 112 | x109/L | (150-450) | |
| WCC | 14.9 | x109/L | (4.0-11.0) | |
|
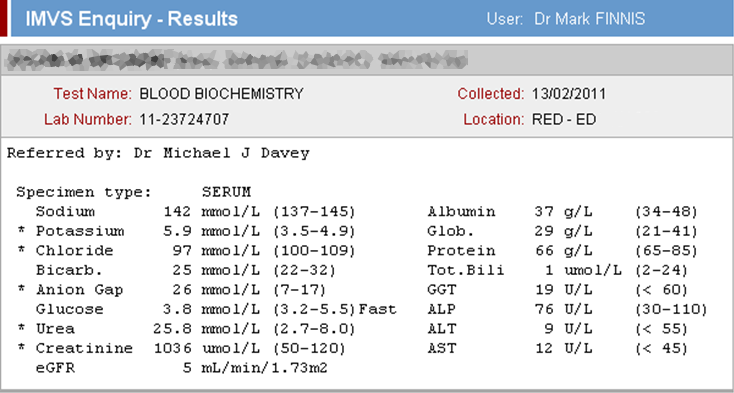
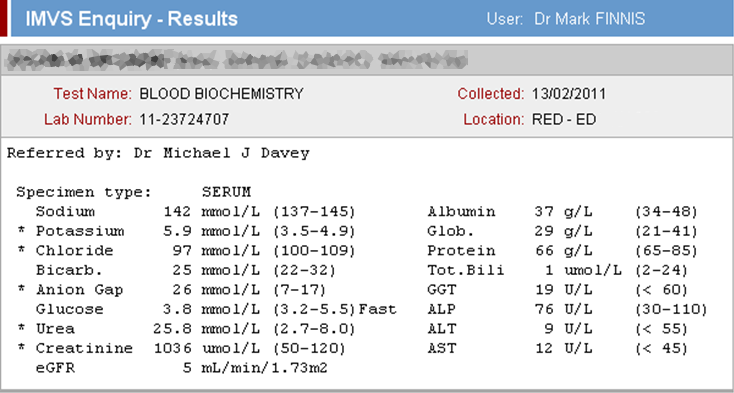
35yo male with longstanding CRF. Weeks of moderate abdominal pain with acute exacerbation. Now depressed LOC/obtundation with acute abdomen & hypotension.
NB: you might reasonably think these aren't real (we did):
|
||||
CRF + GI Bleed/Perforation + Pancreatitis
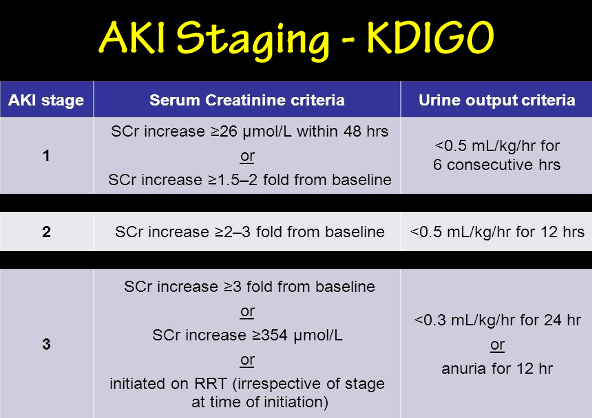
Urea/Creatinine:
NB: hyperkalaemia:
|
||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}