| Specimen | Name | Result | Units | Range |
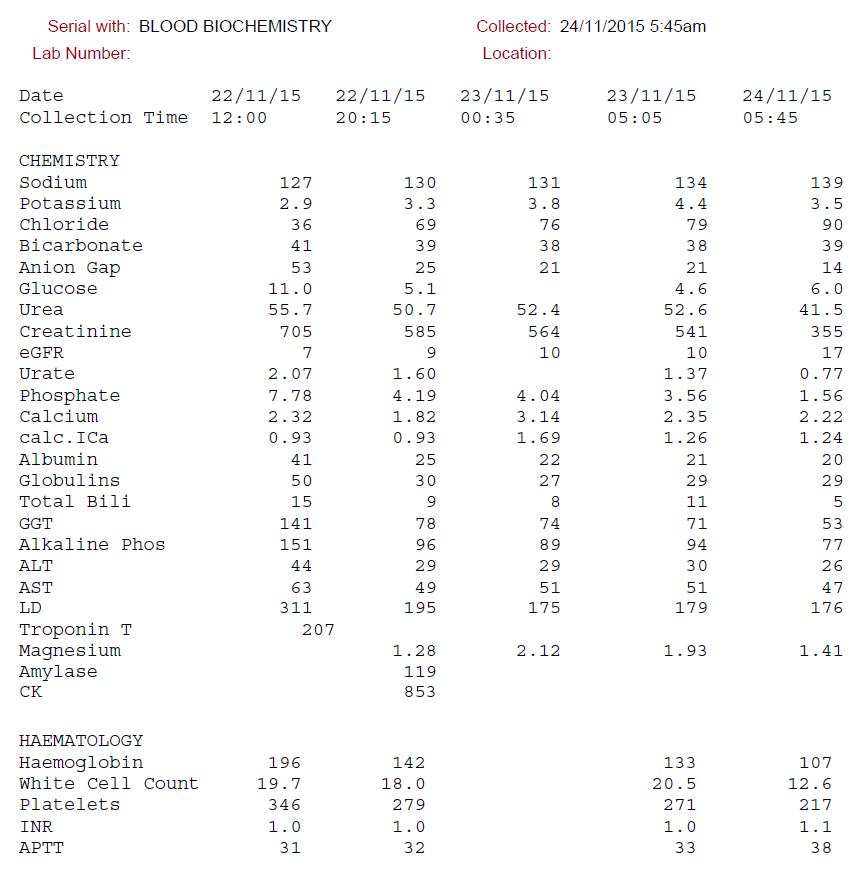
| Plasma | Sodium | 127 | mmol/L | (135-145) |
| Potassium | 2.9 | mmol/L | (3.5-5.5) | |
| Chloride | 36 | mmol/L | (100-109) | |
| Bicarbonate | 41 | mmol/L | (22-32) | |
| Anion Gap | 53 | mmol/L | (7-17) | |
| Glucose | 11.0 | mmol/L | (3.8-5.5) | |
| Urea | 56 | mmol/L | (2.7-7.2) | |
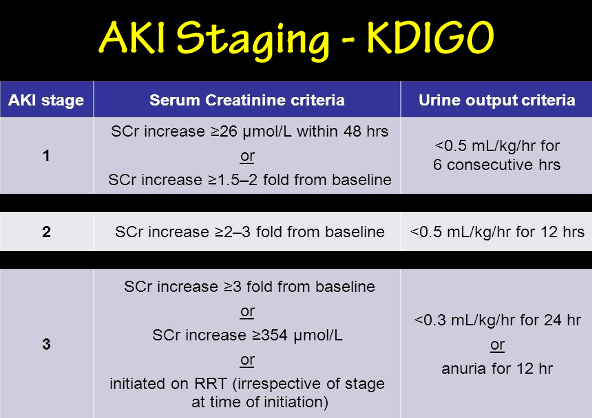
| Creatinine | 705 | μmol/L | (60-110) | |
| Urate | 2.07 | mmol/L | (0.20-0.40) | |
| Phosphate | 7.78 | mmol/L | (0.80-1.45) | |
| Total Calcium | 2.32 | mmol/L | (2.10-2.55) | |
| Albumin | 41 | g/L | (34-48) | |
| Globulins | 50 | g/L | (22-35) | |
| Total Bilirubin | 15 | μmol/L | (6-24) | |
| GGT | 141 | U/L | (< 60) | |
| ALP | 151 | U/L | (30-110) | |
| ALT | 44 | U/L | (< 55) | |
| AST | 63 | U/L | (< 45) | |
| LDH | 311 | U/L | (110-230) | |
| Lipase | 83 | U/L | (< 60) | |
| Blood | Hb | 196 | g/L | (130-180) |
| Platelets | 346 | x109/L | (150-450) | |
| WCC | 19.7 | x109/L | (4.0-11.0) | |
| INR | 1.0 | (0.8-1.2) | ||
| APTT | 31 | Sec. | (25-35) | |
| ABG | pH | 7.49 | (7.36-7.44) | |
| PaO2 | 79 | mmHg | (70-100) | |
| PaCO2 | 61 | mmHg | (35-45) | |
| HCO3- | 46 | mmol/L | (21-26) | |
| Lactate | 2.2 | mmol/L | (< 1.3) | |
|
Homeless 47yo male admitted with depressed LOC / obtundation. Known history of ETOH abuse. Vomiting++ for 1 week prior. |
||||
Complex Mixed PictureUpper GI H+-K+-volume Losses / Hypovolaemia / Hemoconcentration
Likely sequence:
|
||||
{kind=link}
{kind=link}