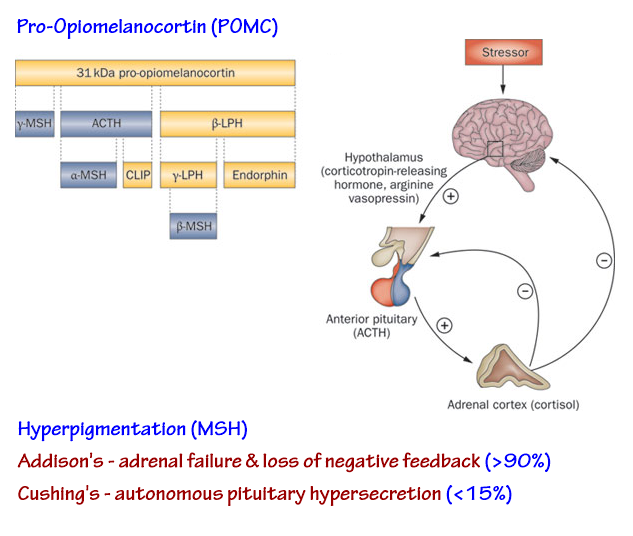
Cushing's Syndrome
- marked hypokalaemic metabolic alkalosis
→ too severe for diuretics, no history of GI losses, ∴ likely endocrine
- ABG → incomplete compensation ≅ respiratory acidosis
*also on supplemental O2
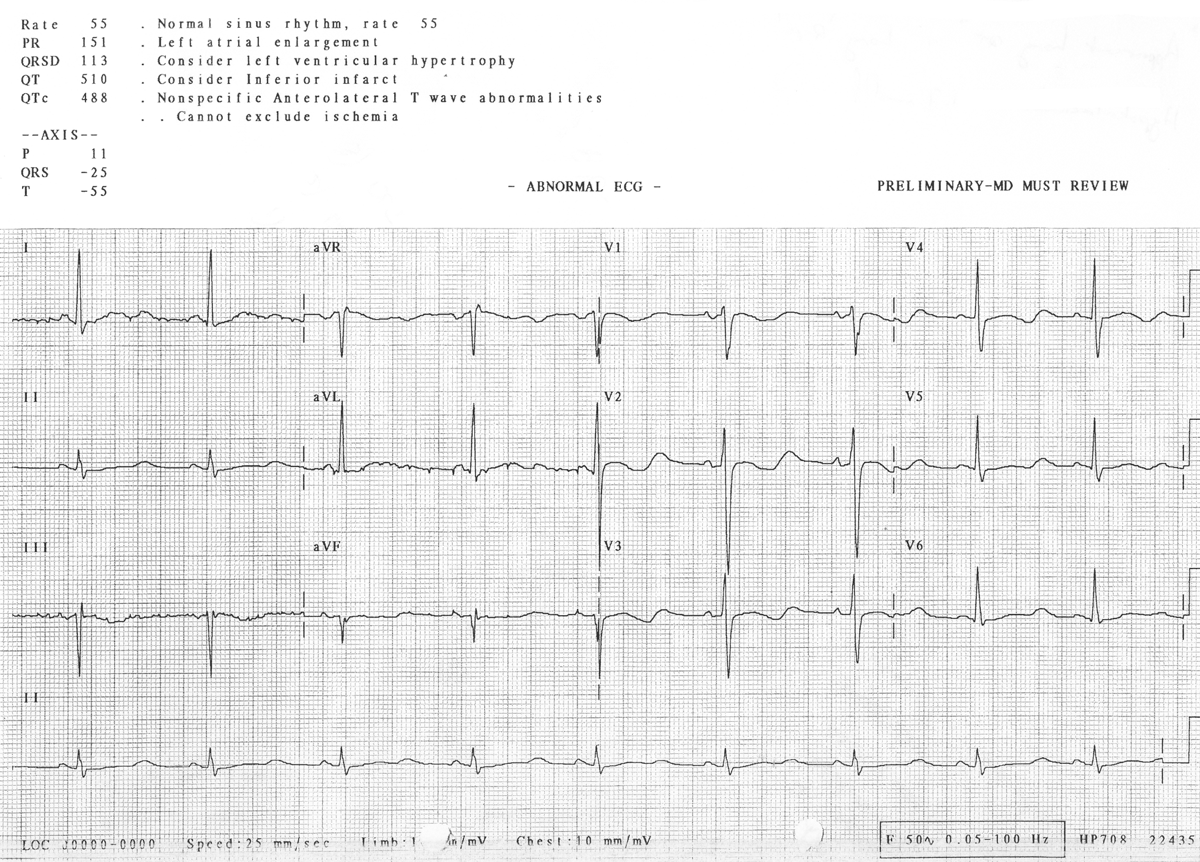
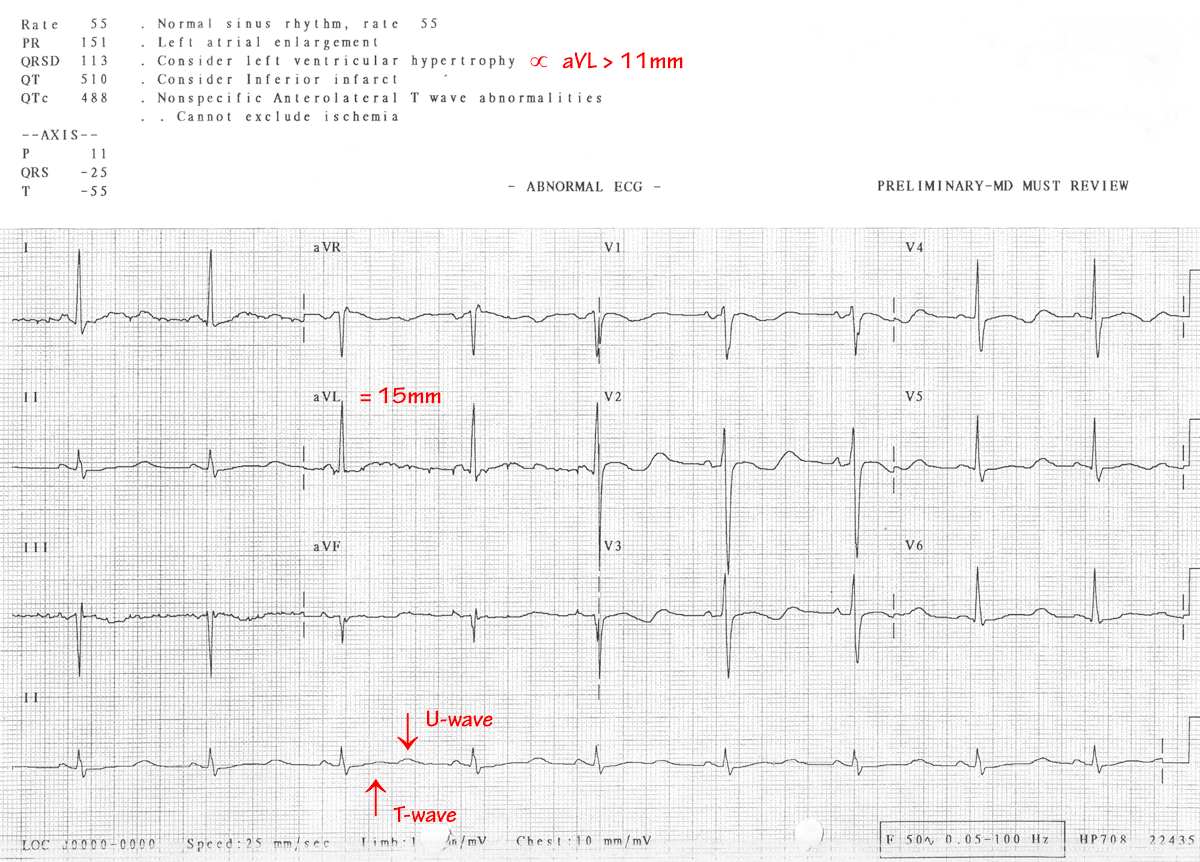
- ECG:
- random cortisol (16:00) ≈ 1542 nmol/L (R: At 17:00 < 250nmol/L)
→ likely hypercortisolaemia but need to adjust for diurnal variation
- 24hr urine free cortisol 528 nmol/24hr (R: 50-350)
→ confirmed hypercortisolaemia but need to ascertain adrenal vs pituitary
- plasma ACTH ≈ 376 ng/L (R: 10-60)
→ confirmed pituitary origin (consistent with pigmentation)
Causes of hypertension and hypokalaemic alkalosis
- Cushing's syndrome
- primary hyperaldosteronism
- essential hypertension & diuretic use
- essential hypertension & 2° hyperaldosteronism
- malignant hypertension
- renovascular hypertension
- drugs - steroids, oestrogen
- renin-secreting tumour
- congenital adrenal enzyme deficiencies
- carbenoxolone
- Liddle's syndrome - 'pseudohyperaldosteronism'
Cushing's Syndrome
- iatrogenic steroid administration → most common
- pituitary adenoma (≈70%) - of remainder
- ectopic ACTH (≈15%) → biochemical effects, not clinically Cushingoid
- adrenal adenoma / carcinoma (≈15%)
- Clinical Features:
- truncal obesity ≈ 90%
- hypertension ≈ 80%
↑renin, ↑vascular reactivity, ↑blood volume 2° fluid retention
- plethoric face ≈ 75%
- hirsutism ≈ 70%
- proximal myopathy ≈ 60%
- osteoporosis ≈ 60%
- bruising, striae ≈ 50%
- poor wound healing ≈ 40%
- NB: usual "ACTH" picture ∝ rate of tumour growth →
- rapidly growing tumours - eg. oat cell
→ hypokalaemia, muscle weakness & wasting, and hyperpigmentation
- slowly growing tumours - e.g. ovary, thyroid medullary, thymic, pancreatic, bronchial adenoma
→ classical Cushingoid features
- Electrolyte Abnormalities
- high Na+, HCO3- & glucose
- low K+ & Ca++
- metabolic alkalosis
- Secondary Endocrine Effects
- insulin resistance / glucose intolerance
- 2° hyperparathyroidism ∝ ↑ urinary Ca++ excretion / ↓ GIT absorption
- antagonism of GH effects
- ↑ACTH → ↑pigmentation
- androgen excess
| Hypokalaemic Metabolic Alkalosis |
|
Diuretics (esp. loop agents) |
- low Na+, Cl- / high urea
|
|
Mineralocorticoid excess |
- normal-high Na+, Cl- / normal urea |
|
Vomiting / Gastric outlet obs. |
- very low Cl- / low-normal Na+ / high urea |
|
Diarrhoea / laxatives |
- low Cl- / normal Na+ / high urea |
|
Post massive transfusion |
- citrate metabolism & acidosis correction |
|
{kind=link}
{kind=link}
{kind=link}
{kind=link}