| Specimen | Name | Result | Units | Range |
| Plasma | Sodium | 115 | mmol/L | (135-145) |
| Potassium | 2.4 | mmol/L | (3.5-5.5) | |
| Chloride | 40 | mmol/L | (100-109) | |
| Bicarbonate | 26 | mmol/L | (22-32) | |
| Anion Gap | 51 | mmol/L | (7-17) | |
| Glucose | 99 | mmol/L | (3.8-5.5) | |
| Urea | 12.3 | mmol/L | (2.7-7.2) | |
| Creatinine | 300 | μmol/L | (60-110) | |
| Urea/Creat Ratio | 41 | (35-80) | ||
| Osmolality | 347 | mmol/kg | (275-295) | |
| Albumin | 36 | g/L | (34-48) | |
| Total Bilirubin | 19 | μmol/L | (6-24) | |
| GGT | 99 | U/L | (< 60) | |
| ALP | 205 | U/L | (30-110) | |
| AST | 18 | U/L | (< 45) | |
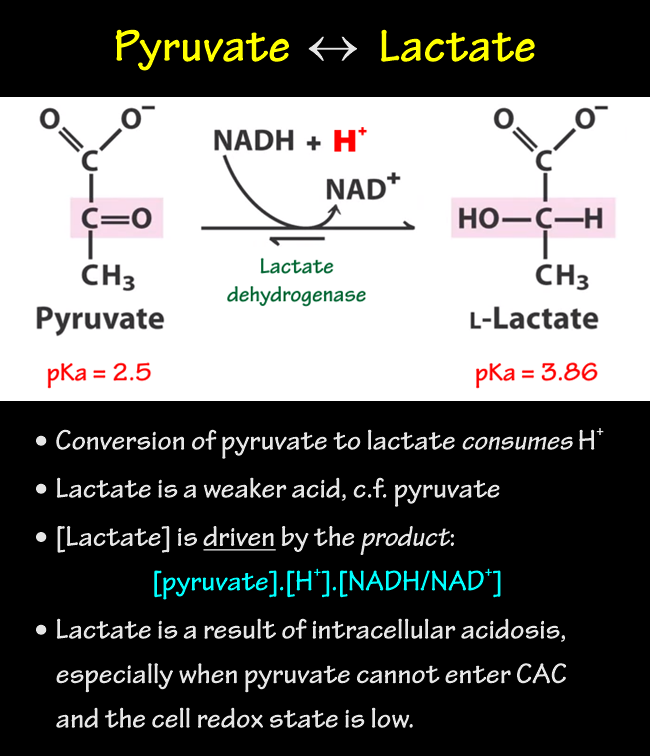
| Lactate | 18 | mmol/L | (< 1.3) | |
| Amylase | 71 | U/L | (20-100) | |
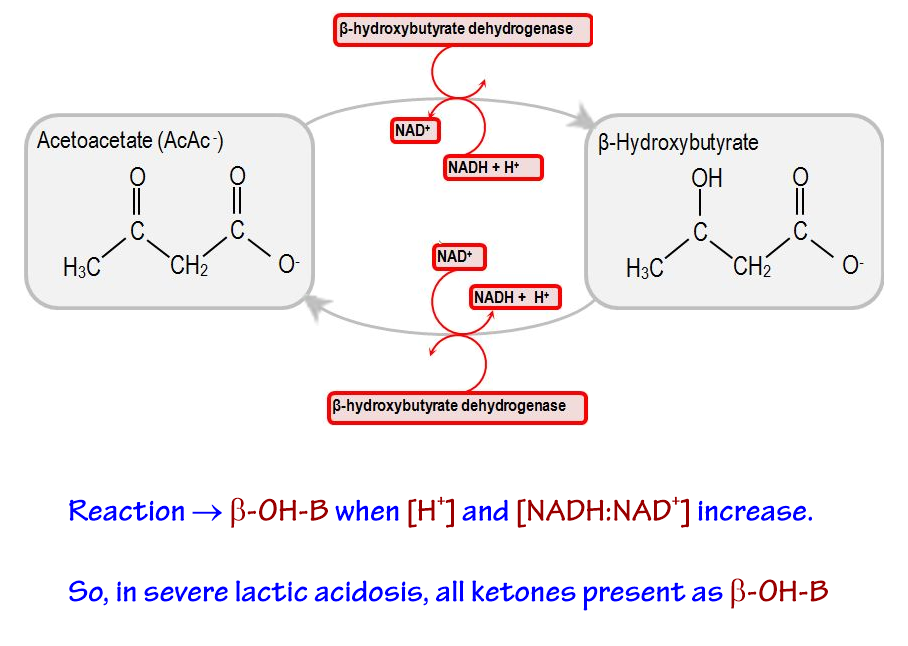
| Beta-hydroxybutyrate | 0.33 | mmol/L | (< 0.09) | |
| Acetoacetate | 0.00 | mmol/L | (< 0.3) | |
| Blood Alcohol | 0.00 | g/dL (%) | (< 0.05) | |
| ABG | pH | 7.42 | (7.36-7.44) | |
| PaO2 | 43 | mmHg | (70-100) | |
| PaCO2 | 57 | mmHg | (35-45) | |
| HCO3- | 38 | mmol/L | (21-26) | |
|
Male 42yo collapsed in the street. PHx: CAL Depressed CNS but able to respond to questioning. BP ≈ 60/- |
||||
Hyperglycaemic Non-ketotic Coma
Complicated biochemical picture:
Hyperosmolar Hyponatraemia:
Differential:
|
||||
{kind=link}
{kind=link}