| Specimen | Name | Result | Units | Range |
| Plasma | Sodium | 142 | mmol/L | (135-145) |
| Potassium | 4.3 | mmol/L | (3.5-5.5) | |
| Chloride | 97 | mmol/L | (100-109) | |
| Bicarbonate | 29 | mmol/L | (22-32) | |
| Anion Gap | 20 | mmol/L | (7-17) | |
| Glucose | 4.1 | mmol/L | (3.8-5.5) | |
| Urea | 4.2 | mmol/L | (2.7-7.2) | |
| Creatinine | 120 | μmol/L | (60-110) | |
| Osmolality | 279 | mmol/kg | (275-295) | |
| Urate | 0.33 | mmol/L | (0.20-0.40) | |
| Phosphate | 1.30 | mmol/L | (0.80-1.45) | |
| Total Calcium | 2.40 | mmol/L | (2.10-2.55) | |
| Albumin | 45 | g/L | (34-48) | |
| Globulins | 26 | g/L | (22-35) | |
| Total Bilirubin | 64 | μmol/L | (6-24) | |
| Conj. Bilirubin | 42 | μmol/L | (1-4) | |
| GGT | 298 | U/L | (< 60) | |
| ALP | 208 | U/L | (30-110) | |
| AST | 17,800 | U/L | (< 45) | |
| LDH | 13,425 | U/L | (110-230) | |
| Cholesterol | 3.4 | mmol/L | (3.5-5.5) | |
|
27yo male with history of chronic headaches & ETOH abuse. |
||||
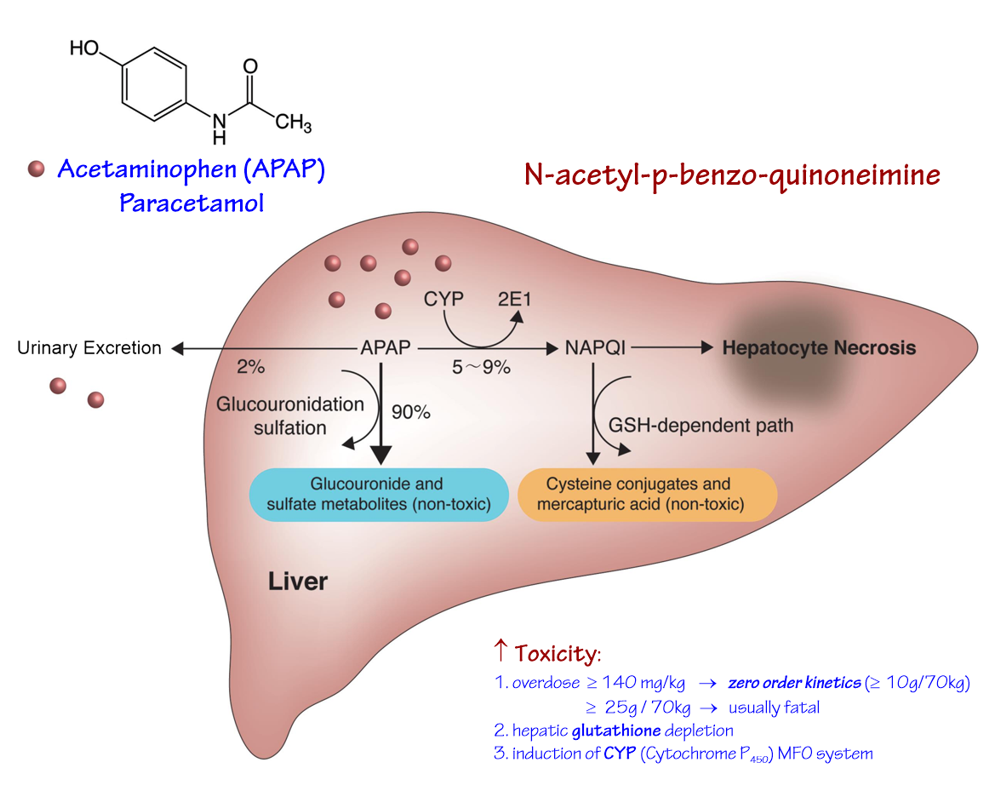
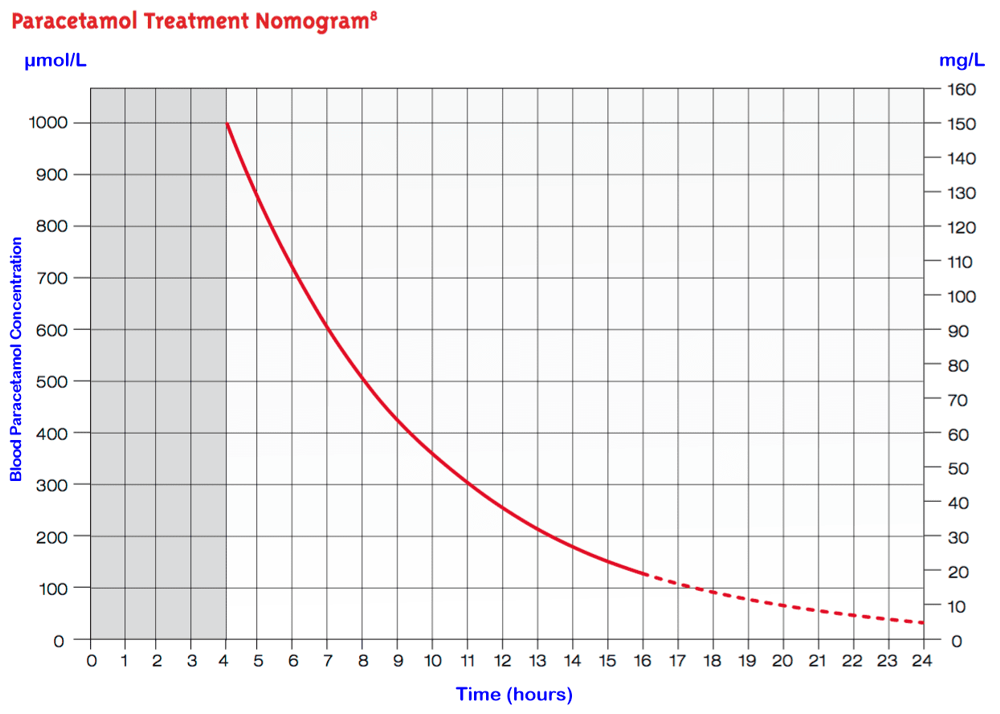
Paracetamol & Alcohol Hepatic Necrosis
Elevation of AST:
Pathogenesis:
Clinical Features:
|
||||
{kind=link}
{kind=link}