| Specimen | Name | Result | Units | Range |
| Plasma | Sodium | 133 | mmol/L | (135-145) |
| Potassium | 9.4 | mmol/L | (3.5-5.5) | |
| Chloride | 102 | mmol/L | (100-109) | |
| Bicarbonate | 6 | mmol/L | (22-32) | |
| Anion Gap | 34 | mmol/L | (7-17) | |
| Glucose | 7.2 | mmol/L | (3.8-5.5) | |
| Urea | 11.0 | mmol/L | (2.7-7.2) | |
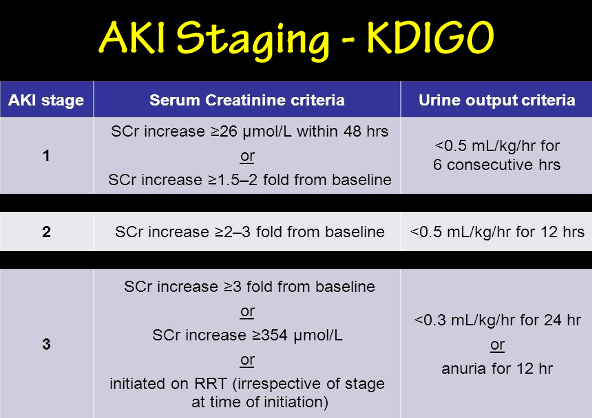
| Creatinine | 290 | μmol/L | (60-110) | |
| Osmolality | 365 | mmol/kg | (275-295) | |
| Urate | 0.54 | mmol/L | (0.20-0.40) | |
| Phosphate | 4.02 | mmol/L | (0.80-1.45) | |
| Total Calcium | 2.17 | mmol/L | (2.10-2.55) | |
| Albumin | 48 | g/L | (34-48) | |
| Globulins | 31 | g/L | (22-35) | |
| Total Bilirubin | 5 | μmol/L | (6-24) | |
| Conj. Bilirubin | 1 | μmol/L | (1-4) | |
| GGT | 50 | U/L | (< 60) | |
| ALP | 124 | U/L | (30-110) | |
| AST | 37 | U/L | (< 45) | |
| LDH | 372 | U/L | (110-230) | |
| Cholesterol | 7.7 | mmol/L | (3.5-5.5) | |
| ABG | pH | 6.77 | (7.36-7.44) | |
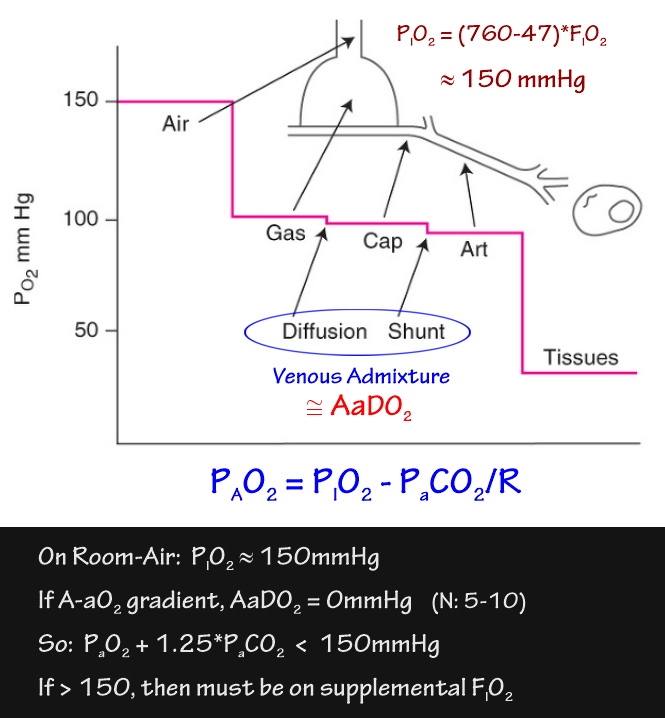
| PaO2 | 149 | mmHg | (70-100) | |
| PaCO2 | 49 | mmHg | (35-45) | |
| HCO3- | 7 | mmol/L | (21-26) | |
|
44yo male admitted unconscious via ED. High O2 requirement: FiO2 > 0.8 |
||||
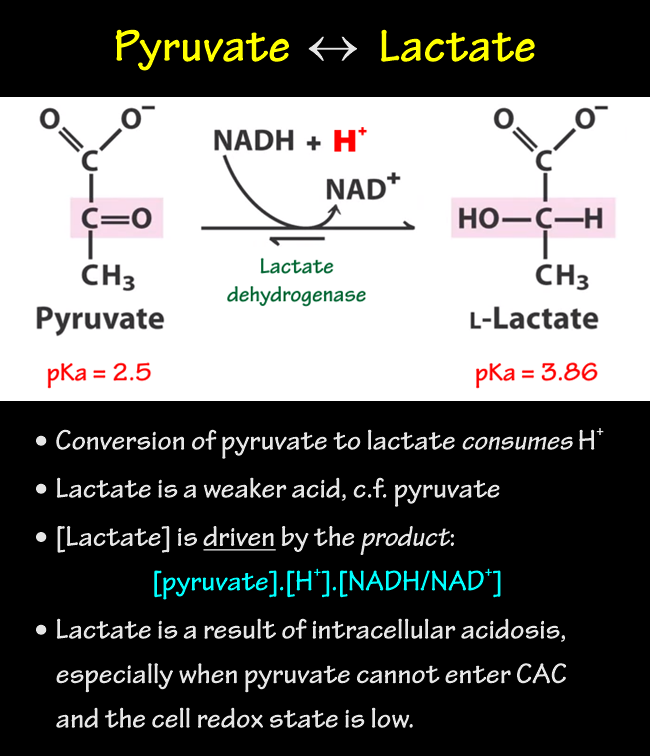
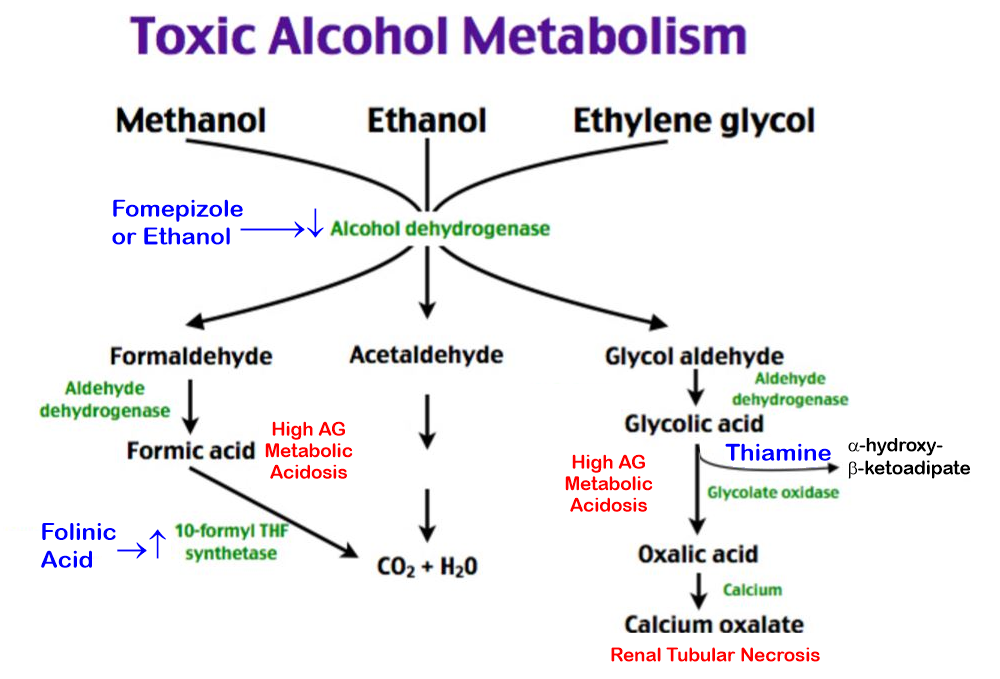
Methanol Overdose
Metabolic Acidosis - Raised Anion Gap (>18)
|
||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}